Health Articles
Skeletal System
The Skeletal System
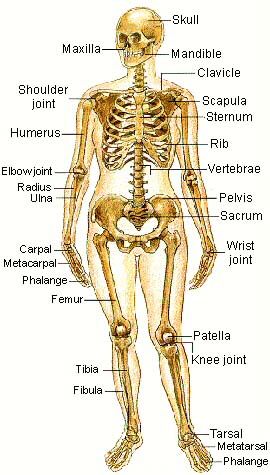 The Skeletal System serves many important functions; it provides the shape and form for our bodies in addition to supporting, protecting, allowing bodily movement, producing blood for the body, and storing minerals.
The Skeletal System serves many important functions; it provides the shape and form for our bodies in addition to supporting, protecting, allowing bodily movement, producing blood for the body, and storing minerals.
Functions
Its 206 bones form a rigid framework to which the softer tissues and organs of the body are attached.
Vital organs are protected by the skeletal system. The brain is protected by the surrounding skull as the heart and lungs are encased by the sternum and rib cage.
Bodily movement is carried out by the interaction of the muscular and skeletal systems. For this reason, they are often grouped together as the musculo-skeletal system. Muscles are connected to bones by tendons. Bones are connected to each other by ligaments. Where bones meet one another is typically called a joint. Muscles which cause movement of a joint are connected to two different bones and contract to pull them together. An example would be the contraction of the biceps and a relaxation of the triceps. This produces a bend at the elbow. The contraction of the triceps and relaxation of the biceps produces the effect of straightening the arm.
Blood cells are produced by the marrow located in some bones. An average of 2.6 million red blood cells are produced each second by the bone marrow to replace those worn out and destroyed by the liver.
Bones serve as a storage area for minerals such as calcium and phosphorus. When an excess is present in the blood, buildup will occur within the bones. When the supply of these minerals within the blood is low, it will be withdrawn from the bones to replenish the supply.
Muscular System
In muscular system there are three different groups
These are three different groups.:
1. SMOOTH MUSCLES - The smooth muscles are muscles that we don't have control of. They include muscles that surround organs including the stomach, lungs, and intestines. Because we cannot control them, they are called "involuntary muscles"
2. SKELETAL MUSCLES - Skeletal muscles are muscles that are directly attached to bones. These muscles are responsible for all of the movement our body can accomplish. When most people think of muscles, they think of skeletal muscles.
3. CARDIAC MUSCLES - Cardiac muscles are only found in one place in your body...your heart. This involuntary set of muscles make up the chambers of your heart. They pump all day and night transporting blood throughout the body.
Muscles are only able to CONTRACT or pull. Because our body has to move in many directions, most muscles are set up in pairs so that one muscle can pull a bone in one direction, and another muscle can pull the bone back the other way.
There are over 600 kinds of muscles that scientists have named. Some muscles are tiny - when we get goosebumps, we are actually seeing a tiny muscle contracting to raise a hair. The longest muscle is satorius muscle in your leg. The largest muscle in the body is Gluteus Maximus - the muscle you sit on!
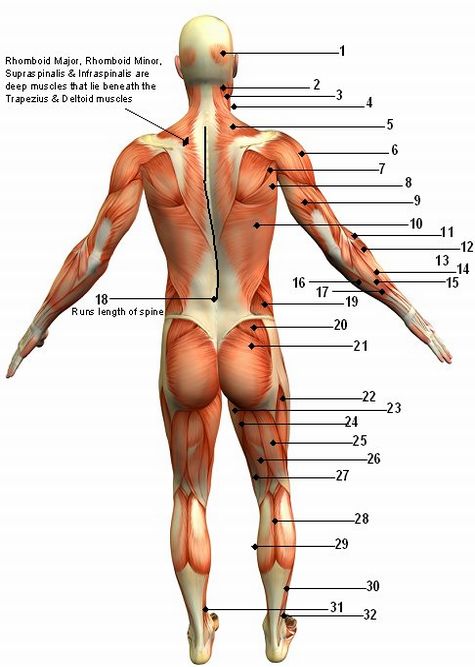
1. Occipitalis
2. Semispinalis Capitis
3. Splenius Capitis
4. Sternocleidomastoid
5. Trapezius
6. Deltiod
7. Teres Minor
8. Teres Major
9. Triceps Brachii
10. Latissimus Dorsi
11. Brachioradialis
12. Extensor Carpi Radialis Longus
13. Anconeus
14. Extensor Carpi Radialis Brevis
15. Extensor Digitorum
16. Flexor Carpi Ulnaris
17 Extensor Carpi Ulnaris
18. Erector Spinae
19. Internal & External Oblique
20. Gluteus Medius & Gluteus Minimus (underneath Gluteus Medius)
21. Gluteus Maximus
22. Vastus Lateralis
23. Gracilis
24. Adductor Magnus
25. Biceps Femoris
26. Semitendinosus
27. Semimembranosus
28. Gastocnemius
29. Soleus
30. Peroneus Longus
31. Flexor Digitorum Longus
32. Extensor Digitorum Longus
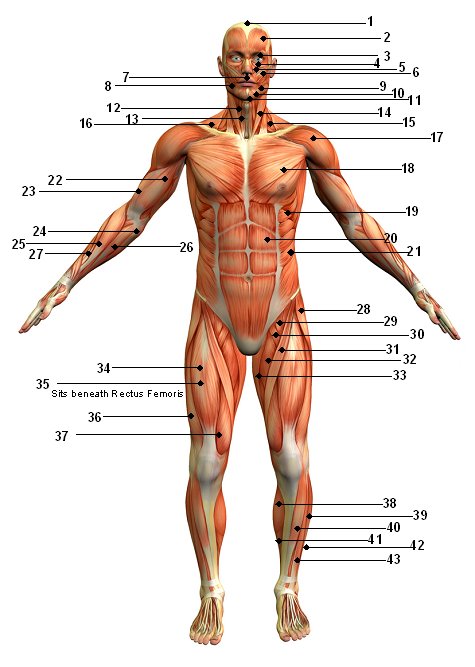
1. Galea Aponeurotica
2. Epicranius
3. Orbicularis Oculi
4. Nasalis
5. Levator Labii Superioris
6. Zygomaticus major & minor
7. Orbicularis Oris
8. Risorius
9. Depressor Anguli Oris
10. Depressor Labii Inferioris
11. Mentalis
12. Omohyoid
13. Sternohyoid
14. Sternal Head of Sternocleidomastoid
15. Scalene
16. Trapezius
17. Deltoid
18. Pectoralis Major
19. Serratus Anterior
20. Rectus Abdominis
21. External Abdominal Oblique
22. Biceps Brachii
23. Brachialis
24. Pronator Teres
25. Brachioradialis
26. Flexor Carpi Radialis
27. Extensor Carpi Radialis
28. Tensor Fasciae Latae
29. Iliopsoas
30. Pectineus
31. Sartorius
32. Adductor Longus
33. Gracilis
34. Rectus Femoris
35. Vastus Intermedius
36. Vastus Lateralis
37. Vastus Medialis
38. Gastrocnemius
39. Peroneus Longus
40. Tibialis Anterior
41. Soleus
42. Peroneus Brevis
43. Extensor Digitorum Longus
Nervous System
As the most complex system, the nervous system serves as the body control center and communications electrical-chemical wiring network. As a key homeostatic regulatory and coordinating system, it detects, interprets, and responds to changes in internal and external conditions. The nervous system integrates countless bits of information and generates appropriate reactions by sending electrochemical impulses through nerves to effector organs such as muscles and glands. The brain and spinal cord are the central nervous system (CNS); the connecting nerve processes to effectors and receptors serve as the peripheral nervous system (PNS). Special sense receptors provide for taste, smell, sight, hearing, and balance. Nerves carry all messages exchanged between the CNS and the rest of the body.
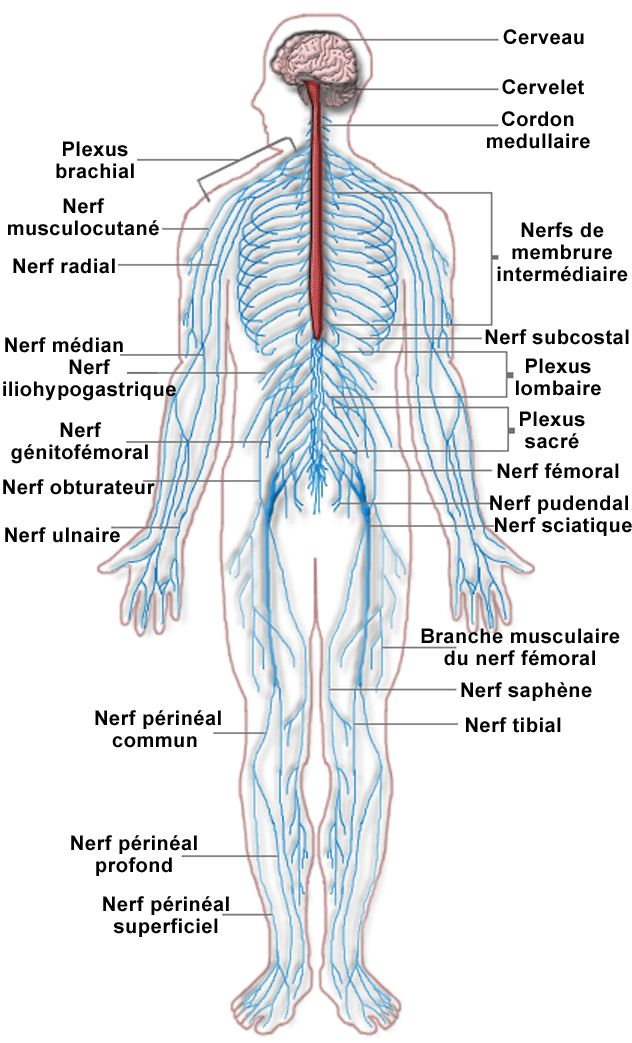
Nervous system: set of nerves, ganglions and nervous centers that receive sensory signal. Commands and coordinates vital functions.
Brachial plexus: network of nerves of the arm.
Intercostal nerve: cord conducting nerve impulses between the ribs.
Radial nerve: cord conducting nerve impulses in the area of the radius.
Median nerve: main cord conducting nerve impulses in the upper limb.
Ulnar nerve: cord conducting nerve impulses in the area of the elbow.
Lumbar plexus: network of nerves of the lower back.
Sciatic nerve: cord conducting nerve impulses in the area of the thigh and lower leg.
Common peroneal nerve: cord conducting nerve impulses along the inside of the lower leg.
Superficial peroneal nerve: cord conducting nerve impulses of the muscles and skin of the leg.
Digital nerve: cord conducting nerve impulses of the fingers.
Sacral plexus: network of nerves of the sacrum.
Spinal cord: substance belonging to the nervous system, found in the holes of the vertebrae.
Cerebellum: nervous centre situated under the brain.
Cerebrum: seat of the mental capacities.
Endocrine System
Although we rarely think about them, the glands of the endocrine system and the hormones they release influence almost every cell, organ, and function of our bodies. The endocrine system is instrumental in regulating mood, growth and development, tissue function, and metabolism, as well as sexual function and reproductive processes.
In general, the endocrine system is in charge of body processes that happen slowly, such as cell growth. Faster processes like breathing and body movement are controlled by the nervous system. But even though the nervous system and endocrine system are separate systems, they often work together to help the body function properly.
About the Endocrine System
The foundations of the endocrine system are the hormones and glands. As the body's chemical messengers, hormones transfer information and instructions from one set of cells to another. Although many different hormones circulate throughout the bloodstream, each one affects only the cells that are genetically programmed to receive and respond to its message. Hormone levels can be influenced by factors such as stress, infection, and changes in the balance of fluid and minerals in blood.
A gland is a group of cells that produces and secretes, or gives off, chemicals. A gland selects and removes materials from the blood, processes them, and secretes the finished chemical product for use somewhere in the body. Some types of glands release their secretions in specific areas. For instance, exocrine glands, such as the sweat and salivary glands, release secretions in the skin or inside of the mouth. Endocrine glands, on the other hand, release more than 20 major hormones directly into the bloodstream where they can be transported to cells in other parts of the body.
The major glands that make up the human endocrine system are the hypothalamus, pituitary, thyroid, parathyroids, adrenals, pineal body, and the reproductive glands, which include the ovaries and testes. The pancreas is also part of this hormone-secreting system, even though it is also associated with the digestive system because it also produces and secretes digestive enzymes.
Although the endocrine glands are the body's main hormone producers, some non-endocrine organs — such as the brain, heart, lungs, kidneys, liver, thymus, skin, and placenta — also produce and release hormones.
The hypothalamus, a collection of specialized cells that is located in the lower central part of the brain, is the primary link between the endocrine and nervous systems. Nerve cells in the hypothalamus control the pituitary gland by producing chemicals that either stimulate or suppress hormone secretions from the pituitary.
Although it is no bigger than a pea, the pituitary gland, located at the base of the brain just beneath the hypothalamus, is considered the most important part of the endocrine system. It's often called the "master gland" because it makes hormones that control several other endocrine glands. The production and secretion of pituitary hormones can be influenced by factors such as emotions and seasonal changes. To accomplish this, the hypothalamus relays information sensed by the brain (such as environmental temperature, light exposure patterns, and feelings) to the pituitary.
The tiny pituitary is divided into two parts: the anterior lobe and the posterior lobe. The anterior lobe regulates the activity of the thyroid, adrenals, and reproductive glands. Among the hormones it produces are:
• growth hormone, which stimulates the growth of bone and other body tissues and plays a role in the body's handling of nutrients and minerals
• prolactin, which activates milk production in women who are breastfeeding
• thyrotropin, which stimulates the thyroid gland to produce thyroid hormones
• corticotropin, which stimulates the adrenal gland to produce certain hormones
The pituitary also secretes endorphins, chemicals that act on the nervous system to reduce sensitivity to pain. In addition, the pituitary secretes hormones that signal the ovaries and testes to make sex hormones. The pituitary gland also controls ovulation and the menstrual cycle in women.
The posterior lobe of the pituitary releases antidiuretic hormone, which helps control body water balance through its effect on the kidneys and urine output; and oxytocin, which triggers the contractions of the uterus that occur during labor.
The thyroid, located in the front part of the lower neck, is shaped like a bowtie or butterfly and produces the thyroid hormones thyroxine and triiodothyronine. These hormones control the rate at which cells burn fuels from food to produce energy. As the level of thyroid hormones increases in the bloodstream, so does the speed at which chemical reactions occur in the body.
Thyroid hormones also play a key role in bone growth and the development of the brain and nervous system in children. The production and release of thyroid hormones is controlled by thyrotropin, which is secreted by the pituitary gland.
Attached to the thyroid are four tiny glands that function together called the parathyroids. They release parathyroid hormone, which regulates the level of calcium in the blood with the help of calcitonin, which is produced in the thyroid.
The body has two triangular adrenal glands, one on top of each kidney. The adrenal glands have two parts, each of which produces a set of hormones and has a different function. The outer part, the adrenal cortex, produces hormones called corticosteroids that influence or regulate salt and water balance in the body, the body's response to stress, metabolism, the immune system, and sexual development and function.
The inner part, the adrenal medulla, produces catecholamines, such as epinephrine. Also called adrenaline, epinephrine increases blood pressure and heart rate when the body experiences stress. (Epinephrine injections are often used to counteract a severe allergic reaction.)
The pineal body, also called the pineal gland, is located in the middle of the brain. It secretes melatonin, a hormone that may help regulate the wake-sleep cycle.
The gonads are the main source of sex hormones. In males, they are located in the scrotum. Male gonads, or testes, secrete hormones called androgens, the most important of which is testosterone. These hormones regulate body changes associated with sexual development, including enlargement of the penis, the growth spurt that occurs during puberty, and the appearance of other male secondary sex characteristics such as deepening of the voice, growth of facial and pubic hair, and the increase in muscle growth and strength. Working with hormones from the pituitary gland, testosterone also supports the production of sperm by the testes.
The female gonads, the ovaries, are located in the pelvis. They produce eggs and secrete the female hormones estrogen and progesterone. Estrogen is involved in the development of female sexual features such as breast growth, the accumulation of body fat around the hips and thighs, and the growth spurt that occurs during puberty. Both estrogen and progesterone are also involved in pregnancy and the regulation of the menstrual cycle.
The pancreas produces (in addition to others) two important hormones, insulin and glucagon. They work together to maintain a steady level of glucose, or sugar, in the blood and to keep the body supplied with fuel to produce and maintain stores of energy.
What the Endocrine System Does
Once a hormone is secreted, it travels from the endocrine gland through the bloodstream to target cells designed to receive its message. Along the way to the target cells, special proteins bind to some of the hormones. The special proteins act as carriers that control the amount of hormone that is available to interact with and affect the target cells.
Also, the target cells have receptors that latch onto only specific hormones, and each hormone has its own receptor, so that each hormone will communicate only with specific target cells that possess receptors for that hormone. When the hormone reaches its target cell, it locks onto the cell's specific receptors and these hormone-receptor combinations transmit chemical instructions to the inner workings of the cell.
When hormone levels reach a certain normal or necessary amount, further secretion is controlled by important body mechanisms to maintain that level of hormone in the blood. This regulation of hormone secretion may involve the hormone itself or another substance in the blood related to the hormone.
For example, if the thyroid gland has secreted adequate amounts of thyroid hormones into the blood, the pituitary gland senses the normal levels of thyroid hormone in the bloodstream and adjusts its release of thyrotropin, the pituitary hormone that stimulates the thyroid gland to produce thyroid hormones.
Another example is parathyroid hormone, which increases the level of calcium in the blood. When the blood calcium level rises, the parathyroid glands sense the change and decrease their secretion of parathyroid hormone. This turnoff process is called a negative feedback system.
Problems With the Endocrine System
Too much or too little of any hormone can be harmful to the body. For example, if the pituitary gland produces too much growth hormone, a child may grow excessively tall. If it produces too little, a child may be abnormally short.
Controlling the production of or replacing specific hormones can treat many endocrine disorders in children and adolescents, some of which include:
Adrenal insufficiency. This condition is characterized by decreased function of the adrenal cortex and the consequent underproduction of adrenal corticosteroid hormones. The symptoms of adrenal insufficiency may include weakness, fatigue, abdominal pain, nausea, dehydration, and skin changes. Doctors treat adrenal insufficiency by giving replacement corticosteroid hormones.
Cushing syndrome. Excessive amounts of glucocorticoid hormones in the body can lead to Cushing syndrome. In children, it most often results when a child takes large doses of synthetic corticosteroid drugs (such as prednisone) to treat autoimmune diseases such as lupus. If the condition is due to a tumor in the pituitary gland that produces excessive amounts of corticotropin and stimulates the adrenals to overproduce corticosteroids, it's known as Cushing disease. Symptoms may take years to develop and include obesity, growth failure, muscle weakness, easy bruising of the skin, acne, high blood pressure, and psychological changes. Depending on the specific cause, doctors may treat this condition with surgery, radiation therapy, chemotherapy, or drugs that block the production of hormones.
Type 1 diabetes. When the pancreas fails to produce enough insulin, type 1 diabetes (previously known as juvenile diabetes) occurs. Symptoms include excessive thirst, hunger, urination, and weight loss. In children and teens, the condition is usually an autoimmune disorder in which specific immune system cells and antibodies produced by the immune system attack and destroy the cells of the pancreas that produce insulin. The disease can cause long-term complications including kidney problems, nerve damage, blindness, and early coronary heart disease and stroke. To control their blood sugar levels and reduce the risk of developing diabetes complications, kids with this condition need regular injections of insulin.
Type 2 diabetes. Unlike type 1 diabetes, in which the body can't produce normal amounts of insulin, in type 2 diabetes the body is unable to respond to insulin normally. Children and teens with the condition tend to be overweight, and it is believed that excess body fat plays a role in the insulin resistance that characterizes the disease. In fact, the rising prevalence of this type of diabetes in kids has paralleled the dramatically increasing rates of obesity among kids in recent years. The symptoms and possible complications of type 2 diabetes are basically the same as those of type 1. Some kids and teens can control their blood sugar level with dietary changes, exercise, and oral medications, but many will need to take insulin injections like patients with type 1 diabetes.
Growth hormone problems. Too much growth hormone in children who are still growing will make their bones and other body parts grow excessively, resulting in gigantism. This rare condition is usually caused by a pituitary tumor and can be treated by removing the tumor. In contrast, when the pituitary gland fails to produce adequate amounts of growth hormone, a child's growth in height is impaired. Hypoglycemia (low blood sugar) may also occur in kids with growth hormone deficiency, particularly in infants and young children with the condition.
Hyperthyroidism. Hyperthyroidism is a condition in which the levels of thyroid hormones in the blood are excessively high. Symptoms may include weight loss, nervousness, tremors, excessive sweating, increased heart rate and blood pressure, protruding eyes, and a swelling in the neck from an enlarged thyroid gland (goiter). In kids the condition is usually caused by Graves' disease, an autoimmune disorder in which specific antibodies produced by the immune system stimulate the thyroid gland to become overactive. The disease may be controlled with medications or by removal or destruction of the thyroid gland through surgery or radiation treatments.
Hypothyroidism. Hypothyroidism is a condition in which the levels of thyroid hormones in the blood are abnormally low. Thyroid hormone deficiency slows body processes and may lead to fatigue, a slow heart rate, dry skin, weight gain, constipation, and, in kids, slowing of growth and delayed puberty. Hashimoto's thyroiditis, which results from an autoimmune process that damages the thyroid and blocks thyroid hormone production, is the most common cause of hypothyroidism in kids. Infants can also be born with an absent or underdeveloped thyroid gland, resulting in hypothyroidism. It can be treated with oral thyroid hormone replacement.
Precocious puberty. Body changes associated with puberty may occur at an abnormally young age in some kids if the pituitary hormones that stimulate the gonads to produce sex hormones rise prematurely. An injectable medication is available that can suppress the secretion of these pituitary hormones (known as gonadotropins) and arrest the progression of sexual development in most of these children.
Puberty, usually occurring during adolescence, is when kids develop physically and emotionally into young men and women. Usually, this starts to happen no earlier than about 7 to 8 years of age for girls and 9 years of age for boys (the average age is about 10 for girls and 12 for boys). But what if a younger child - for example, a 5-year-old girl - begins showing the signs of puberty? How would it affect her?
Precocious puberty - the onset of signs of puberty before age 7 or 8 in girls and age 9 in boys - can be physically and emotionally difficult for children and can sometimes be the sign of an underlying health problem.
Precocious Puberty
What are the Signs of Precocious Puberty?
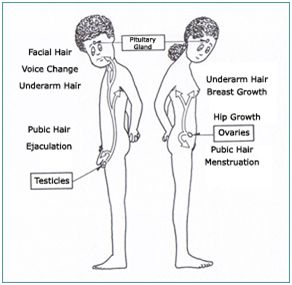
In girls, the telltale signs of precocious puberty include any of the following before 7 or 8 years of age:
• breast development
• pubic or underarm hair development
• rapid height growth - a growth "spurt"
• onset of menstruation
• acne
• "mature" body odor
In boys, the signs of precocious puberty before 9 years of age include:
• enlargement of the testicles or penis
• pubic, underarm, or facial hair development
• rapid height growth - a growth "spurt"
• voice deepening
• acne
• "mature" body odor
Many children who show some of the early signs of puberty have what's known as "partial" precocious puberty. Some girls, usually beginning between the ages of 6 months and 3 years, may show breast development that later disappears or may persist without other physical changes of puberty.
Similarly, some girls and boys may experience early growth of pubic and/or underarm hair that isn't associated with other changes in sexual development. Children with "partial" precocious puberty may require evaluation to rule out "true" precocious puberty or other health problems, but they generally need no treatment and usually will show the other expected signs of puberty at the usual age.
How Does Precocious Puberty Affect a Child?
When puberty ends, growth in height stops. Because their skeletons mature and bone growth stops at an earlier age than normal, kids with precocious puberty usually don't achieve their full adult height potential. Their early growth spurt may make them initially tall when compared with their peers, but they may stop growing too soon and end up at a shorter height than they would have otherwise.
Going through puberty early can also be difficult for a child emotionally and socially. For example, girls with precocious puberty may be confused or embarrassed about physical changes such as getting their periods or having enlarged breasts well before any of their peers. But the hardest part may be the teasing that children with the condition - especially girls - may experience.
Even emotions and behavior may change in children with precocious puberty. Girls can become moody and irritable. Boys can become more aggressive and also develop a sex drive inappropriate for their age.
What Causes Precocious Puberty?
The onset of puberty is normally triggered by the hypothalamus (the area of the brain that helps control pituitary gland function). It signals the pituitary gland (a pea-sized gland near the base of the brain) to release hormones that stimulate the ovaries (in girls) or testicles (in boys) to make sex hormones.
Sometimes, precocious puberty stems from a structural problem in the brain (such as a tumor), brain injury due to head trauma, an infection (such as meningitis), or a problem in the ovaries or thyroid gland that triggers the onset of puberty ahead of schedule - but this usually isn't the case.
For the majority of girls, there's no underlying medical problem - they simply start puberty too early for no known reason. In boys, the condition is less common, and more likely to be associated with an underlying medical problem than it is in girls.
In about 5% of boys, precocious puberty is inherited. Starting puberty early can be passed to the son from the father or to the son from the maternal grandfather through the mother (who will not be affected by the disorder). But less than 1% of girls affected by precocious puberty have inherited the condition.
How Is Precocious Puberty Diagnosed?
Talk to your child's doctor if your child shows any signs of early sexual maturation before age 7 or 8 in girls or age 9 in boys, including breast development, rapid height growth, menstruation, acne, enlarged testicles or penis, or pubic or underarm hair.
The physical changes boys and girls go through during puberty are usually evident to a doctor during an exam. To confirm a diagnosis of precocious puberty, your child's doctor may order blood and urine tests to detect elevated levels of sex hormones. And X-rays of your child's wrist and hand can show whether the bones are maturing too rapidly.
Imaging and scanning tests such as CT scans, MRIs (magnetic resonance imaging), and ultrasound studies can help rule out specific causes of precocious puberty, such as a tumor in the brain, ovary, or testicle.
How Is Precocious Puberty Treated?
If your child's doctor suspects that your little one has precocious puberty, he or she may refer you to a pediatric endocrinologist (a doctor who specializes in growth and hormonal disorders in children) for further evaluation and treatment.
Once it's diagnosed, the goal of treating precocious puberty is to halt or even reverse sexual development and stop the rapid growth and bone maturation that can eventually result in adult short stature. Depending upon the cause, there are two possible approaches to treatment:
1. treating the underlying cause or disease, such as a tumor
2. lowering the high levels of sex hormones with medication to stop sexual development from progressing
In some cases, treatment of an underlying health problem can stop the precocious puberty from progressing. But in most cases, because there's no other disease triggering the condition, treatment usually consists of hormone therapy that stops sexual development.
The currently approved hormone treatment is with drugs called LHRH analogs - synthetic hormones that block the body's production of the sex hormones that are causing the early puberty. Dramatic results are usually seen within a year of starting treatment with an LHRH analog, which is generally safe and usually causes no side effects in children. In girls, breast size may decrease - or at least there will be no further development. In boys, the penis and testicles may shrink back to the size expected for their age. Growth in height will also slow down to a rate expected for children before puberty. A child's behavior usually becomes more age appropriate as well.
Caring for Your Child
Give your child a simple, truthful explanation about what's happening. Explain that these changes are normal for older kids and teens, but that his or her body has started developing a little too early. Keep your child informed about his or her treatment and what can be expected along the way.
Also be sure to watch for signs that teasing or other difficulties associated with precocious puberty may be affecting your child's emotional development. Common warning signs to discuss with your child's doctor include:
• poor grades
• problems at school
• loss of interest in daily activities
• depression
How you cope with the issue can also determine how successfully your child will cope. The goal is to prevent your child from dwelling on sexual development or developing a poor self-image or low self-esteem. To create a supportive environment, try not to focus your comments on your child's appearance; instead, offer praise for achievements in school or sports and support your child's participation in other activities.
The important thing to remember is that children with precocious puberty can be treated. Doctors can help your child preserve his or her adult height potential as well as limit the emotional and social difficulties your child may face from maturing early.
About Puberty
What is Puberty?
Puberty is the time when your body starts to change from that of a child to that of an adult. Going from childhood to adulthood is not just a bodily process many other changes will accompany it.
Many changes occur during this time and hormones bring on these changes. Hormones are chemicals released by the brain, as the brain knows when the body is reaching sexual, physical and intellectual maturity. Different types of hormones are responsible for different changes occurring in you. The hormones that bring on the onset of puberty come from a gland near the brain called the pituitary gland. There are hormones that promote the production of other hormones called estrogen and progesterone in girls’ ovaries and in boys the hormonetestoterone is produced in the testicles.
During this period growth of hormones become active as well, these are responsible for the physical changes that occur in your body. Your body will grow taller you will gain weight
and your shape will change in a general way as well. It is important to know that not everybody experiences these changes at the same time; some people's ‘growth spurt’ might come earlier or later than others and might vary in degrees.
Other types of hormones that affect you during this period are those responsible for the emotional changes. These could generate feelings of confusion, sadness, mood swings and possibly a quick temper. You may experience varying positive or negative feelings and these too are provoked by hormonal changes. You might also feel more self-conscious and possibly socially isolated. It is important to understand that this is normal. These feelings may vary in severity between different people. The best way to deal with this is to talk to someone you trust, choose a family member you can communicate with. Your mother, your aunt, your father or an older sibling could be the best person to talk to, remember that your family is there to support you in all your needs. Communicating with people who care for you is very important, it can help clear much of the confusion you are feeling and can help you look at things from a different perspective.
Emotional changes:
Puberty is not just about physical changes; emotional changes are a big part of this period and these two go together. You might be feeling more self-conscious about the physical changes you are going through. It is important to try not to compare your development with others your age as every person is a unique individual with special needs and problems and his/her development is specific to him/her.
As you are moving from being a young girl or young boy to becoming a woman or a man, your thinking is changing as well. Your relationships, interests, priorities and your world and the important people in it will change as well. This may sound easy but it is not always so. It is important to realize that you are not alone in this and it is not impossible for caring adults in your family to understand what you are going through.
Those crazy hormones are acting up again and they bring on these emotional changes again. Following are some of the emotional changes you might experience during this time:
- You may feel confused.
- You may develop very strong emotions.
- You may feel sad.
- You might have frequent mood changes.
- You might be over sensitive.
- You might get angry and lose your temper more easily.
- You might experience a sense of not belonging to your family, friends etc.
- You might experience problems at school.
- You may ask yourself is it normal to feel what you are feeling.
Yes it is normal to feel this way, you might experience some or most of these emotional symptoms. When matters become too hard to deal with on your own, you have to remember that there are many people who love and care for you no matter what you are going through. Try to approach a person in your family you trust and feel comfortable enough to address these issues with. You will notice how much better you will feel when you share the burden of these emotions with someone you trust. Remember that all adults have gone through this before even your parents.
When does puberty happen?
Puberty is a process that does not follow a strict timeline and it affects each person according to his or her own internal calendar; although it generally starts earlier for girls than boys.
Puberty for girls can begin between ages nine and fourteen, for boys it will be between the ages of ten and seventeen. These age brackets are considered as the norm though anything happening slightly before or after this could still be considered normal. This development process can last from one year to as many as six years. For some it might be a rather quick process or an early one for some it might happen later and take longer.
In the following section we will talk about the physical changes that happen during puberty.
Cardiovascular System
The cardiovascular system is sometimes called the blood-vascular or simply the circulatory system. It consists of the heart, which is a muscular pumping device, and a closed system of vessels called arteries, veins, and capillaries. As the name implies, blood contained in the circulatory system is pumped by the heart around a closed circle or circuit of vessels as it passes again and again through the various "circulations" of the body.
As in the adult, survival of the developing embryo depends on the circulation of blood to maintain homeostasis and a favorable cellular environment. In response to this need, the cardiovascular system makes its appearance early in development and reaches a functional state long before any other major organ system. Incredible as it seems, the primitive heart begins to beat regularly early in the fourth week following fertilization.
The vital role of the cardiovascular system in maintaining homeostasis depends on the continuous and controlled movement of blood through the thousands of miles of capillaries that permeate every tissue and reach every cell in the body. It is in the microscopic capillaries that blood performs its ultimate transport function. Nutrients and other essential materials pass from capillary blood into fluids surrounding the cells as waste products are removed.
Numerous control mechanisms help to regulate and integrate the diverse functions and component parts of the cardiovascular system in order to supply blood to specific body areas according to need. These mechanisms ensure a constant internal environment surrounding each body cell regardless of differing demands for nutrients or production of waste products.
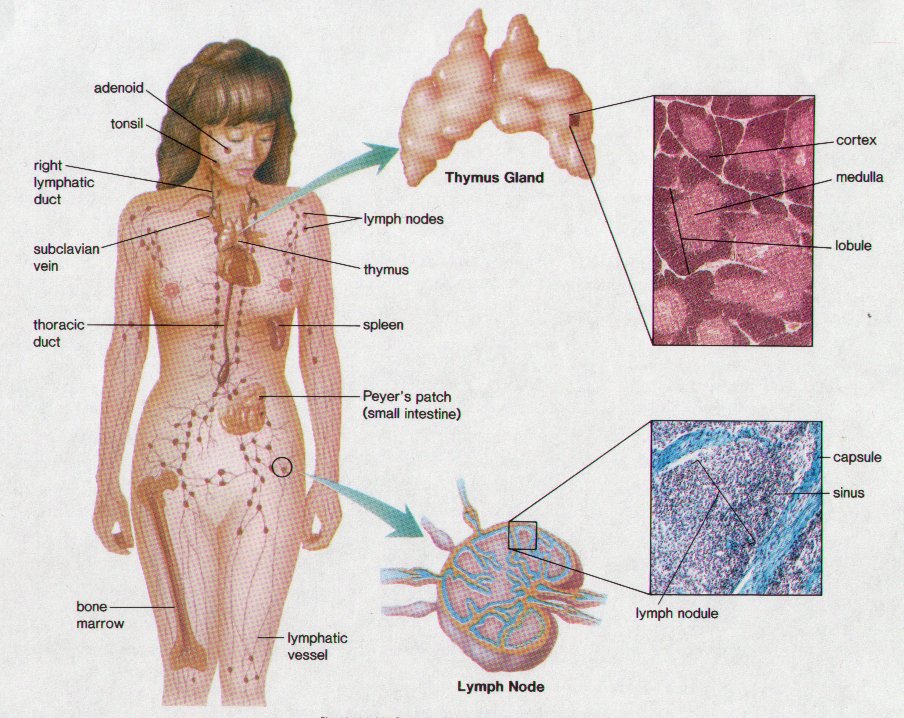
Lymphatic system
The lymphatic system is a network of tubes throughout the body that drains fluid (called lymph) from tissues and empties it back into the bloodstream. The main roles of the lymphatic system include managing the fluid levels in the body, filtering out bacteria, and housing types of white blood cells. Lymph is filtered through the spleen, thymus and lymph nodes before being emptied into the blood.
Keeping a balance of fluid
Blood vessels tend to seep fluid into surrounding tissue. The lymphatic system drains off any extra fluid to stop the tissues from puffing up. The feet in particular are prone to puffiness.
Lymphatic vessels
Lymphatic vessels criss-cross the entire body, except for the central nervous system. Some lymphatic vessels have valves (similar to the valves in veins), which stop the lymph from running back the wrong way.
Spleen
The spleen is inside the abdomen, just under the diaphragm. This is one of the filtering organs of the blood. As well as removing microbes, the spleen also destroys old or damaged red blood cells.
Thymus
The thymus is inside the ribcage, just behind the breastbone. This is another filtering organ of the blood, that contains many white blood cells called lymphocytes.
Lymph nodes
Lymph nodes are found at various points around the body, including the throat, armpits, chest, abdomen and groin. All lie close to arteries. Bacteria picked up from the tissues by the lymph are trapped in the lymph node. White blood cells called lymphocytes can then attack and kill the bacteria. This is why your lymph nodes tend to swell if you have an infection. Viruses and cancer cells are also trapped by lymph nodes.
Common problems
Some common problems of the lymphatic system include:
• Glandular fever - symptoms include tender lymph nodes
• Hodgkin’s disease - a type of cancer of the lymphatic system
• Oedema - swelling caused by too much fluid in the tissues
• Tonsillitis - infection of the tonsils in the throat.
Things to remember
• The lymphatic system maintains fluid levels in the body.
• Bacteria and other microbes are taken up by the lymph and delivered to the lymph nodes for destruction.
• The spleen and thymus are organs that filter the blood.
Digestive System
The digestive system is made up of the digestive tract—a series of hollow organs joined in a long, twisting tube from the mouth to the anus—and other organs that help the body break down and absorb food (see figure).
Organs that make up the digestive tract are the mouth, esophagus, stomach, small intestine, large intestine—also called the colon—rectum, and anus. Inside these hollow organs is a lining called the mucosa. In the mouth, stomach, and small intestine, the mucosa contains tiny glands that produce juices to help digest food. The digestive tract also contains a layer of smooth muscle that helps break down food and move it along the tract.
Two “solid” digestive organs, the liver and the pancreas, produce digestive juices that reach the intestine through small tubes called ducts. The gallbladder stores the liver’s digestive juices until they are needed in the intestine. Parts of the nervous and circulatory systems also play major roles in the digestive system.
Why is digestion important?
When you eat foods—such as bread, meat, and vegetables—they are not in a form that the body can use as nourishment. Food and drink must be changed into smaller molecules of nutrients before they can be absorbed into the blood and carried to cells throughout the body. Digestion is the process by which food and drink are broken down into their smallest parts so the body can use them to build and nourish cells and to provide energy.
How is food digested?
Digestion involves mixing food with digestive juices, moving it through the digestive tract, and breaking down large molecules of food into smaller molecules. Digestion begins in the mouth, when you chew and swallow, and is completed in the small intestine.
Movement of Food Through the System
The large, hollow organs of the digestive tract contain a layer of muscle that enables their walls to move. The movement of organ walls can propel food and liquid through the system and also can mix the contents within each organ. Food moves from one organ to the next through muscle action called peristalsis. Peristalsis looks like an ocean wave traveling through the muscle. The muscle of the organ contracts to create a narrowing and then propels the narrowed portion slowly down the length of the organ. These waves of narrowing push the food and fluid in front of them through each hollow organ.
The first major muscle movement occurs when food or liquid is swallowed. Although you are able to start swallowing by choice, once the swallow begins, it becomes involuntary and proceeds under the control of the nerves.
Swallowed food is pushed into the esophagus, which connects the throat above with the stomach below. At the junction of the esophagus and stomach, there is a ringlike muscle, called the lower esophageal sphincter, closing the passage between the two organs. As food approaches the closed sphincter, the sphincter relaxes and allows the food to pass through to the stomach.
The stomach has three mechanical tasks. First, it stores the swallowed food and liquid. To do this, the muscle of the upper part of the stomach relaxes to accept large volumes of swallowed material. The second job is to mix up the food, liquid, and digestive juice produced by the stomach. The lower part of the stomach mixes these materials by its muscle action. The third task of the stomach is to empty its contents slowly into the small intestine.
Several factors affect emptying of the stomach, including the kind of food and the degree of muscle action of the emptying stomach and the small intestine. Carbohydrates, for example, spend the least amount of time in the stomach, while protein stays in the stomach longer, and fats the longest. As the food dissolves into the juices from the pancreas, liver, and intestine, the contents of the intestine are mixed and pushed forward to allow further digestion.
Finally, the digested nutrients are absorbed through the intestinal walls and transported throughout the body. The waste products of this process include undigested parts of the food, known as fiber, and older cells that have been shed from the mucosa. These materials are pushed into the colon, where they remain until the feces are expelled by a bowel movement.
Production of Digestive Juices
The digestive glands that act first are in the mouth—the salivary glands. Saliva produced by these glands contains an enzyme that begins to digest the starch from food into smaller molecules. An enzyme is a substance that speeds up chemical reactions in the body.
The next set of digestive glands is in the stomach lining. They produce stomach acid and an enzyme that digests protein. A thick mucus layer coats the mucosa and helps keep the acidic digestive juice from dissolving the tissue of the stomach itself. In most people, the stomach mucosa is able to resist the juice, although food and other tissues of the body cannot.
After the stomach empties the food and juice mixture into the small intestine, the juices of two other digestive organs mix with the food. One of these organs, the pancreas, produces a juice that contains a wide array of enzymes to break down the carbohydrate, fat, and protein in food. Other enzymes that are active in the process come from glands in the wall of the intestine.
The second organ, the liver, produces yet another digestive juice—bile. Bile is stored between meals in the gallbladder. At mealtime, it is squeezed out of the gallbladder, through the bile ducts, and into the intestine to mix with the fat in food. The bile acids dissolve fat into the watery contents of the intestine, much like detergents that dissolve grease from a frying pan. After fat is dissolved, it is digested by enzymes from the pancreas and the lining of the intestine.
Absorption and Transport of Nutrients
Most digested molecules of food, as well as water and minerals, are absorbed through the small intestine. The mucosa of the small intestine contains many folds that are covered with tiny fingerlike projections called villi. In turn, the villi are covered with microscopic projections called microvilli. These structures create a vast surface area through which nutrients can be absorbed. Specialized cells allow absorbed materials to cross the mucosa into the blood, where they are carried off in the bloodstream to other parts of the body for storage or further chemical change. This part of the process varies with different types of nutrients.
Carbohydrates. The Dietary Guidelines for Americans 2005 recommend that 45 to 65 percent of total daily calories be from carbohydrates. Foods rich in carbohydrates include bread, potatoes, dried peas and beans, rice, pasta, fruits, and vegetables. Many of these foods contain both starch and fiber.
The digestible carbohydrates—starch and sugar—are broken into simpler molecules by enzymes in the saliva, in juice produced by the pancreas, and in the lining of the small intestine. Starch is digested in two steps. First, an enzyme in the saliva and pancreatic juice breaks the starch into molecules called maltose. Then an enzyme in the lining of the small intestine splits the maltose into glucose molecules that can be absorbed into the blood. Glucose is carried through the bloodstream to the liver, where it is stored or used to provide energy for the work of the body.
Sugars are digested in one step. An enzyme in the lining of the small intestine digests sucrose, also known as table sugar, into glucose and fructose, which are absorbed through the intestine into the blood. Milk contains another type of sugar, lactose, which is changed into absorbable molecules by another enzyme in the intestinal lining.
Fiber is undigestible and moves through the digestive tract without being broken down by enzymes. Many foods contain both soluble and insoluble fiber. Soluble fiber dissolves easily in water and takes on a soft, gel-like texture in the intestines. Insoluble fiber, on the other hand, passes essentially unchanged through the intestines.
Protein. Foods such as meat, eggs, and beans consist of giant molecules of protein that must be digested by enzymes before they can be used to build and repair body tissues. An enzyme in the juice of the stomach starts the digestion of swallowed protein. Then in the small intestine, several enzymes from the pancreatic juice and the lining of the intestine complete the breakdown of huge protein molecules into small molecules called amino acids. These small molecules can be absorbed through the small intestine into the blood and then be carried to all parts of the body to build the walls and other parts of cells.
Fats. Fat molecules are a rich source of energy for the body. The first step in digestion of a fat such as butter is to dissolve it into the watery content of the intestine. The bile acids produced by the liver dissolve fat into tiny droplets and allow pancreatic and intestinal enzymes to break the large fat molecules into smaller ones. Some of these small molecules are fatty acids and cholesterol. The bile acids combine with the fatty acids and cholesterol and help these molecules move into the cells of the mucosa. In these cells the small molecules are formed back into large ones, most of which pass into vessels called lymphatics near the intestine. These small vessels carry the reformed fat to the veins of the chest, and the blood carries the fat to storage depots in different parts of the body.
Vitamins. Another vital part of food that is absorbed through the small intestine are vitamins. The two types of vitamins are classified by the fluid in which they can be dissolved: water-soluble vitamins (all the B vitamins and vitamin C) and fat-soluble vitamins (vitamins A, D, E, and K). Fat-soluble vitamins are stored in the liver and fatty tissue of the body, whereas water-soluble vitamins are not easily stored and excess amounts are flushed out in the urine.
Water and salt. Most of the material absorbed through the small intestine is water in which salt is dissolved. The salt and water come from the food and liquid you swallow and the juices secreted by the many digestive glands.
How is the digestive process controlled?
Hormone Regulators
The major hormones that control the functions of the digestive system are produced and released by cells in the mucosa of the stomach and small intestine. These hormones are released into the blood of the digestive tract, travel back to the heart and through the arteries, and return to the digestive system where they stimulate digestive juices and cause organ movement.
The main hormones that control digestion are gastrin, secretin, and cholecystokinin (CCK):
• Gastrin causes the stomach to produce an acid for dissolving and digesting some foods. Gastrin is also necessary for normal cell growth in the lining of the stomach, small intestine, and colon.
• Secretin causes the pancreas to send out a digestive juice that is rich in bicarbonate. The bicarbonate helps neutralize the acidic stomach contents as they enter the small intestine. Secretin also stimulates the stomach to produce pepsin, an enzyme that digests protein, and stimulates the liver to produce bile.
• CCK causes the pancreas to produce the enzymes of pancreatic juice, and causes the gallbladder to empty. It also promotes normal cell growth of the pancreas.
Additional hormones in the digestive system regulate appetite:
• Ghrelin is produced in the stomach and upper intestine in the absence of food in the digestive system and stimulates appetite.
• Peptide YY is produced in the digestive tract in response to a meal in the system and inhibits appetite.
Both of these hormones work on the brain to help regulate the intake of food for energy. Researchers are studying other hormones that may play a part in inhibiting appetite, including glucagon-like peptide-1 (GPL-1), oxyntomodulin (+ ), and pancreatic polypeptide.
Nerve Regulators
Two types of nerves help control the action of the digestive system.
Extrinsic, or outside, nerves come to the digestive organs from the brain or the spinal cord. They release two chemicals, acetylcholine and adrenaline. Acetylcholine causes the muscle layer of the digestive organs to squeeze with more force and increase the “push” of food and juice through the digestive tract. It also causes the stomach and pancreas to produce more digestive juice. Adrenaline has the opposite effect. It relaxes the muscle of the stomach and intestine and decreases the flow of blood to these organs, slowing or stopping digestion.
The intrinsic, or inside, nerves make up a very dense network embedded in the walls of the esophagus, stomach, small intestine, and colon. The intrinsic nerves are triggered to act when the walls of the hollow organs are stretched by food. They release many different substances that speed up or delay the movement of food and the production of juices by the digestive organs.
Together, nerves, hormones, the blood, and the organs of the digestive system conduct the complex tasks of digesting and absorbing nutrients from the foods and liquids you consume each day.
Urinary System
How does the urinary system work?
Your body takes nutrients from food and uses them to maintain all bodily functions including energy and self-repair. After your body has taken what it needs from the food, waste products are left behind in the blood and in the bowel. The urinary system works with the lungs, skin, and intestines—all of which also excrete wastes—to keep the chemicals and water in your body balanced. Adults eliminate about a quart and a half of urine each day. The amount depends on many factors, especially the amounts of fluid and food a person consumes and how much fluid is lost through sweat and breathing. Certain types of medications can also affect the amount of urine eliminated.
The urinary system removes a type of waste called urea from your blood. Urea is produced when foods containing protein, such as meat, poultry, and certain vegetables, are broken down in the body. Urea is carried in the bloodstream to the kidneys.
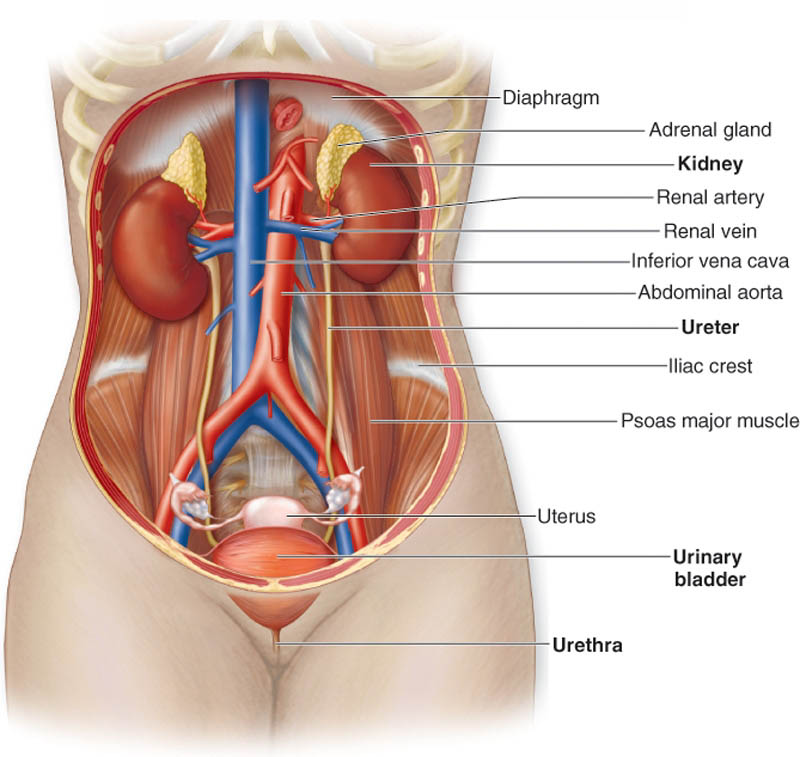
The kidneys are bean-shaped organs about the size of your fists. They are near the middle of the back, just below the rib cage. The kidneys remove urea from the blood through tiny filtering units called nephrons. Each nephron consists of a ball formed of small blood capillaries, called a glomerulus, and a small tube called a renal tubule. Urea, together with water and other waste substances, forms the urine as it passes through the nephrons and down the renal tubules of the kidney.
From the kidneys, urine travels down two thin tubes called ureters to the bladder. The ureters are about 8 to 10 inches long. Muscles in the ureter walls constantly tighten and relax to force urine downward away from the kidneys. If urine is allowed to stand still, or back up, a kidney infection can develop. Small amounts of urine are emptied into the bladder from the ureters about every 10 to 15 seconds.
The bladder is a hollow muscular organ shaped like a balloon. It sits in your pelvis and is held in place by ligaments attached to other organs and the pelvic bones. The bladder stores urine until you are ready to go to the bathroom to empty it. It swells into a round shape when it is full and gets smaller when empty. If the urinary system is healthy, the bladder can hold up to 16 ounces (2 cups) of urine comfortably for 2 to 5 hours.
Circular muscles called sphincters help keep urine from leaking. The sphincter muscles close tightly like a rubber band around the opening of the bladder into the urethra, the tube that allows urine to pass outside the body.
Nerves in the bladder tell you when it is time to urinate, or empty your bladder. As the bladder first fills with urine, you may notice a feeling that you need to urinate. The sensation to urinate becomes stronger as the bladder continues to fill and reaches its limit. At that point, nerves from the bladder send a message to the brain that the bladder is full, and your urge to empty your bladder intensifies.
When you urinate, the brain signals the bladder muscles to tighten, squeezing urine out of the bladder. At the same time, the brain signals the sphincter muscles to relax. As these muscles relax, urine exits the bladder through the urethra. When all the signals occur in the correct order, normal urination occurs.
What causes problems in the urinary system?
Problems in the urinary system can be caused by aging, illness, or injury. As you get older, changes in the kidneys’ structure cause them to lose some of their ability to remove wastes from the blood. Also, the muscles in your ureters, bladder, and urethra tend to lose some of their strength. You may have more urinary infections because the bladder muscles do not tighten enough to empty your bladder completely. A decrease in strength of muscles of the sphincters and the pelvis can also cause incontinence, the unwanted leakage of urine. Illness or injury can also prevent the kidneys from filtering the blood completely or block the passage of urine.
How are problems in the urinary system detected?
Urinalysis is a test that studies the content of urine for abnormal substances such as protein or signs of infection. This test involves urinating into a special container and leaving the sample to be studied.
Urodynamic tests evaluate the storage of urine in the bladder and the flow of urine from the bladder through the urethra. Your doctor may want to do a urodynamic test if you are having symptoms that suggest problems with the muscles or nerves of your lower urinary system and pelvis—ureters, bladder, urethra, and sphincter muscles.
Urodynamic tests measure the contraction of the bladder muscle as it fills and empties. The test is done by inserting a small tube called a catheter through your urethra into your bladder to fill it either with water or a gas. Another small tube is inserted into your rectum or vagina to measure the pressure put on your bladder when you strain or cough. Other bladder tests use x-ray dye instead of water so that x-ray pictures can be taken when the bladder fills and empties to detect any abnormalities in the shape and function of the bladder. These tests take about an hour.
What are some disorders of the urinary system?
Disorders of the urinary system range in severity from easy to treat to life threatening.
Benign prostatic hyperplasia (BPH) is a condition in men that affects the prostate gland, which is part of the male reproductive system. The prostate is located at the bottom of the bladder and surrounds the urethra. BPH is an enlargement of the prostate gland that can interfere with urinary function in older men. It causes blockage by squeezing the urethra, which can make it difficult to urinate. Men with BPH frequently have other bladder symptoms including an increase in frequency of bladder emptying both during the day and at night. Most men over age 60 have some BPH, but not all have problems with blockage. There are many different treatment options for BPH.
Painful bladder syndrome/Interstitial cystitis (PBS/IC) is a chronic bladder disorder also known as frequency-urgency-dysuria syndrome. In this disorder, the bladder wall can become inflamed and irritated. The inflammation can lead to scarring and stiffening of the bladder, decreased bladder capacity, pinpoint bleeding, and, in rare cases, ulcers in the bladder lining. The cause of IC is unknown at this time.
Kidney stones is the term commonly used to refer to stones, or calculi, in the urinary system. Stones form in the kidneys and may be found anywhere in the urinary system. They vary in size. Some stones cause great pain while others cause very little. The aim of treatment is to remove the stones, prevent infection, and prevent recurrence. Both nonsurgical and surgical treatments are used. Kidney stones affect men more often than women.
Prostatitis is inflammation of the prostate gland that results in urinary frequency and urgency, burning or painful urination, a condition called dysuria, and pain in the lower back and genital area, among other symptoms. In some cases, prostatitis is caused by bacterial infection and can be treated with antibiotics. But the more common forms of prostatitis are not associated with any known infecting organism. Antibiotics are often ineffective in treating the nonbacterial forms of prostatitis.
Proteinuria is the presence of abnormal amounts of protein in the urine. Healthy kidneys take wastes out of the blood but leave in protein. Protein in the urine does not cause a problem by itself. But it may be a sign that your kidneys are not working properly.
Renal (kidney) failure results when the kidneys are not able to regulate water and chemicals in the body or remove waste products from your blood. Acute renal failure (ARF) is the sudden onset of kidney failure. This condition can be caused by an accident that injures the kidneys, loss of a lot of blood, or some drugs or poisons. ARF may lead to permanent loss of kidney function. But if the kidneys are not seriously damaged, they may recover. Chronic kidney disease (CKD) is the gradual reduction of kidney function that may lead to permanent kidney failure, or end-stage renal disease (ESRD). You may go several years without knowing you have CKD.
Urinary tract infections (UTIs) are caused by bacteria in the urinary tract. Women get UTIs more often than men. UTIs are treated with antibiotics. Drinking lots of fluids also helps by flushing out the bacteria.
The name of the UTI depends on its location in the urinary tract. An infection in the bladder is called cystitis. If the infection is in one or both of the kidneys, the infection is called pyelonephritis. This type of UTI can cause serious damage to the kidneys if it is not adequately treated.
Urinary incontinence, loss of bladder control, is the involuntary passage of urine. There are many causes and types of incontinence, and many treatment options. Treatments range from simple exercises to surgery. Women are affected by urinary incontinence more often than men.
Urinary retention, or bladder-emptying problems, is a common urological problem with many possible causes. Normally, urination can be initiated voluntarily and the bladder empties completely. Urinary retention is the abnormal holding of urine in the bladder. Acute urinary retention is the sudden inability to urinate, causing pain and discomfort. Causes can include an obstruction in the urinary system, stress, or neurologic problems. Chronic urinary retention refers to the persistent presence of urine left in the bladder after incomplete emptying. Common causes of chronic urinary retention are bladder muscle failure, nerve damage, or obstructions in the urinary tract. Treatment for urinary retention depends on the cause.
Who can help me with a urinary problem?
Your primary doctor can help you with some urinary problems. Your pediatrician may be able to treat some of your child’s urinary problems. But some problems may require the attention of a urologist, a doctor who specializes in treating problems of the urinary system and the male reproductive system. A gynecologist is a doctor who specializes in the female reproductive system and may be able to help with some urinary problems. A urogynecologist is a gynecologist who specializes in the female urinary system. A nephrologist specializes in treating diseases of the kidney.
Points to Remember
• Your urinary system filters waste and extra fluid from your blood.
• Problems in the urinary system include kidney failure, urinary tract infections, kidney stones, prostate enlargement, and bladder control problems.
• Health professionals who treat urinary problems include general practitioners (your primary doctor), pediatricians, urologists, gynecologists, urogynecologists, and nephrologists.
Advertise With Us
Latest Health News
- Microsoft says AI system better than doctors at diagnosing complex health conditions - The Guardian
- Is private health insurance worth it? What to weigh up at tax time - Australian Broadcasting Corporation
- Students sudden death shocks Adelaide community - The Advertiser
- 'We're deeply sorry': Bupa apologises for misleading consumers, repays millions of dollars - Australian Broadcasting Corporation
- How AI chatbots are delivering health lies to 'millions' - 9News